
The ASCO Post is pleased to present Hematology Expert Review, an ongoing feature that occasionally quizzes readers on issues in hematology. In this installment, Drs. Abutalib, Pemmaraju, and Medeiros highlight the clinically aggressive blastic plasmacytoid dendritic cell neoplasm. For each quiz question that follows, select the one best answer. The correct answers and accompanying discussions follow.
GUEST EDITORS

Dr. Abutalib is Associate Director of the Hematology and Cellular Therapy Program and Director, Clinical Apheresis Program, Cancer Treatment Centers of America, Zion, Illinois; Associate Professor at Rosalind Franklin University of Medicine and Science; and Founder and Co-Editor-in-Chief of Advances in Cell & Gene Therapy. Dr. Pemmaraju is Associate Professor, Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston. Dr. Medeiros is Professor and Chair of the Department of Hematopathology at The University of Texas MD Anderson Cancer Center.
Question 1
Which of the following statements about blastic plasmacytoid dendritic cell neoplasm is correct?
A. It does not affect mucosal surfaces.
B. It is associated with Epstein-Barr virus infection.
C. It does not involve the lymph nodes.
D. The skin is frequently involved.
Question 2
Which of the following disease(s) is/are associated with blastic plasmacytoid dendritic cell neoplasm?
A. Acute myeloid leukemia (AML)
B. Myelodysplastic syndromes (MDS)
C. Chronic myelomonocytic leukemia (CMML)
D. All of the above
Question 3
How is mature plasmacytoid dendritic cell proliferation distinguished from blastic plasmacytoid dendritic cell neoplasm?
A. In most cases of mature plasmacytoid dendritic cell proliferation, plasmacytoid dendritic cells are CD56-negative.
B. Plasmacytoid dendritic cells express terminal deoxynucleotidyl transferase in mature plasmacytoid dendritic cell proliferation but not in blastic plasmacytoid dendritic cell neoplasm.
C. Mature plasmacytoid dendritic cell proliferation is not associated with an underlying myeloid malignancy.
D. All of the above
Question 4
Which of the following sets of four markers would establish the diagnosis of blastic plasmacytoid dendritic cell neoplasm?
A. CD4, TCF-4, CD303, TCL-1
B. CD4, CD56, CD123, CD303
C. TCL-1, CD2AP, CD123, CD303
D. All of the above
Question 5
Which of the following antigens is a therapeutic target in blastic plasmacytoid dendritic cell neoplasm?
A. CD303
B. CD123
C. CD56
D. CD4
Answers to Hematology Expert Review Questions
Question 1
Which of the following statements about blastic plasmacytoid dendritic cell neoplasm is correct?
Correct answer: D. The skin is frequently involved.
Expert Perspective
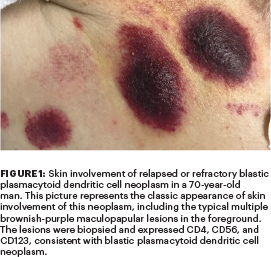
Blastic plasmacytoid dendritic cell neoplasm is a clinically aggressive cancer with a high frequency of cutaneous (64%–100%; Figure 1), bone marrow/peripheral blood (60%–90%; Figure 2), and lymph node (40%–50%) involvement. Other sites also can be involved, including the oral mucosa and the central nervous system.1,2 Blastic plasmacytoid dendritic cell neoplasm is a disorder of immature plasmacytoid dendritic cells; their normal counterpart cells regulate effector T-cell function.1 Solitary or multiple skin lesions are the most frequent clinical presentation (Figure 1). Blastic plasmacytoid dendritic cell neoplasm is not associated with Epstein-Barr virus infection.1
Question 2
Which of the following disease(s) is/are associated with blastic plasmacytoid dendritic cell neoplasm?
Correct answer: D. All of the above.
Expert Perspective
About 10% to 20% of cases of blastic plasmacytoid dendritic cell neoplasm are associated with or develop into other myeloid neoplasms, most commonly CMML but also MDS or AML.1-3 In addition, a few myeloid hematologic neoplasms can share morphologic and immunophenotypic features with blastic plasmacytoid dendritic cell neoplasm, especially AML with monocytic differentiation, which can express CD4, CD56, and CD123.1
Question 3
How is mature plasmacytoid dendritic cell proliferation distinguished from blastic plasmacytoid dendritic cell neoplasm?
Correct answer: A. In most cases of mature plasmacytoid dendritic cell proliferation, plasmacytoid dendritic cells are CD56-negative.
Expert Perspective
Blastic plasmacytoid dendritic cell neoplasm must be distinguished from mature plasmacytoid dendritic cell proliferation, in which plasmacytoid dendritic cells (PDCs) are morphologically mature and, in most cases, negative for CD56 expression or show only focal and weak reactivity.1,4,5 Of note, a minority (8%) of cases of blastic plasmacytoid dendritic cell neoplasm may be negative for CD56 or CD4, which does not exclude the diagnosis, provided other PDC-associated antigens (particularly CD123, TCL-1, or CD303) are expressed. Mature plasmacytoid dendritic cell proliferation is characterized by a low Ki67 proliferation index (< 10%) and lack terminal deoxynucleotidyl transferase (TdT). In the blastic neoplasm, TdT is positive in about one-third of cases (multilineage potential), with expression in 10% to 80% of the cells, and Ki67 proliferation index is between 20% and 80%. Mature plasmacytoid dendritic cell proliferation is invariably associated with a myeloid malignancy—most commonly CMML, MDS, or AML.1

Question 4
Which of the following sets of four markers would establish the diagnosis of blastic plasmacytoid dendritic cell neoplasm?
Correct answer: D. All of the above.
Expert Perspective
All seven markers mentioned (CD2AP, CD4, CD56, CD123, CD303, TCF-4, and TCL-1) are expressed by PDCs.1-6 The diagnosis of blastic plasmacytoid dendritic cell neoplasm requires high clinical suspicion in the appropriate clinical context (Figure 1) and expression of a specific set of markers by immunohistochemistry and/or flow cytometry. Of note, blastic plasmacytoid dendritic cell neoplasms are negative for CD3 (T-cell marker), CD14, CD16 (NK-cell marker), CD20 (B-cell marker), CD34, lysozyme, and myeloperoxidase.1-6
Question 5
Which of the following antigens is a therapeutic target in blastic plasmacytoid dendritic cell neoplasm?
Correct answer: B. CD123.
Expert Perspective
Ubiquitous CD123 (interleukin-3 receptor subunit α) overexpression is characteristic of blastic plasmacytoid dendritic cell neoplasm. This was the basis for investigating the use of tagraxofusp, a CD123-targeted diphtheria immunotoxin.7 Tagraxofusp-erzs is the first U.S. Food and Drug Administration–approved treatment for patients 2 years and older with blastic plasmacytoid dendritic cell neoplasm. It has been shown to be safe and effective in treatment-naive and previously treated adults, with high rates of subsequent allogeneic hematopoietic cell transplantation, particularly in the front-line setting.7,8 The most common treatment-related toxicities are transaminitis and thrombocytopenia, generally observed with the first cycle of therapy. The most serious treatment-related toxicity is capillary leak syndrome.7,8
DISCLOSURE: Dr. Abutalib is an advisor for AstraZeneca. Dr. Pemmaraju has received honoraria from AbbVie, Blueprint Medicines, Celgene, DAVA Oncology, Incyte, LFB Biotechnologies, MustangBio, Novartis, Roche Molecular Diagnostics, and Stemline Therapeutics; has served as a consultant or advisor to Pacylex Pharmaceuticals; has received research funding/grants from AbbVie, Affymetrix/Thermo Fisher Scientific, Cellectis, Daiichi Sankyo, Novartis, Plexxikon, SagerStrong Foundation, Samus Therapeutics, and Stemline Therapeutics; and has been reimbursed for travel, accommodations, or other expenses by AbbVie, Celgene, DAVA Oncology, MustangBio, and Stemline Therapeutics. Dr. Medeiros reported no conflicts of interest.
REFERENCES
1. Facchetti F, Petrella T, Pileri SA: Blastic plasmacytoid dendritic cell neoplasm, in Swerdlow SH, Campo E, Harris NL, et al (eds.): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, pp 174-177. Lyon, France, International Agency for Research in Cancer, 2017.
2. Vitte F, Fabiani B, Bénet C, et al: Specific skin lesions in chronic myelomonocytic leukemia. Am J Surg Pathol 36:1302-1316, 2012.
3. Julia F, Dalle S, Duru G, et al: Blastic plasmacytoid dendritic cell neoplasms: Clinico-immunohistochemical correlations in a series of 91 patients. Am J Surg Pathol 38:673-680, 2014.
4. Assaf C, Gellrich S, Whittaker S, et al: CD56-positive haematological neoplasms of the skin. J Clin Pathol 60:981-989, 2007.
5. Facchetti F, Vermi W, Santoro A, et al: Neoplasms derived from plasmacytoid monocytes/interferon-producing cells. Am J Surg Pathol 27:1489-1493, 2003.
6. Sukswai N, Aung PP, Yin CC, et al: Dual expression of TCF4 and CD123 is highly sensitive and specific for blastic plasmacytoid dendritic cell neoplasm. Am J Surg Pathol 43:1429-1437, 2019.
7. Hammond D, Pemmaraju N: Tagraxofusp for blastic plasmacytoid dendritic cell neoplasm. Hematol Oncol Clin North Am 34:565-574, 2020.
8. Pemmaraju N, Lane AA, Sweet KL, et al: Tagraxofusp in blastic plasmacytoid dendritic-cell neoplasm. N Engl J Med 380:1628-1637, 2019.