
The ASCO Post is pleased to present Hematology Expert Review, an ongoing feature that quizzes readers on issues in hematology. In this installment, Drs. Syed Ali Abutalib and L. Jeffrey Medeiros explore the World Health Organization (WHO) classification of hematopoietic and lymphoid tissue malignancies, focusing on early T-cell precursor acute lymphoblastic leukemia (ETP-ALL). For each quiz question that follows, select the one best answer. The correct answers and accompanying discussions appear below.
GUEST EDITORS

Syed Ali Abutalib, MD

L. Jeffrey Medeiros, MD
Dr. Abutalib is Assistant Director, Hematology and Hematopoietic Cell Transplantation; Director, Hematopoietic Cell Transplant Apheresis Service, Cancer Treatment Centers of America, Zion, Illinois; Founder and Co–Editor-in-Chief, Advances in Cell & Gene Therapy. Dr. Medeiros is Professor and Chair, Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston.
Introduction
The 2016 revision of WHO classification added a provisional entity designated as early T-cell precursor lymphoblastic leukemia. This entity was fully accepted as a distinct entity in the current 5th edition of the WHO classification, designated as early T-precursor lymphoblastic leukemia/lymphoma. We use the abbreviation ETP-ALL for simplicity. This disease is associated with more aggressive behavior compared with other subtypes of T-cell ALL/lymphoblastic lymphoma. It accounts for 15% of T-cell ALL in children and about 35% of adult cases.
Question 1
Which of the following statements about immunophenotype in ETP-ALL is correct?
A. These leukemias are positive for surface CD3.
B. These leukemias do not express stem cell or myeloid-associated markers.
C. These leukemias do not express CD1a or CD8.
D. All of the above.
Question 2
Which statement about the ETP-ALL cell of origin is correct?
A. The leukemia is derived from T-cell precursors in the bone marrow.
B. The leukemia stem cells are committed to the T-cell lineage.
C. The leukemia is derived from T-cell precursors in the thymus.
D. B and C.
Question 3
Which statement about oncologic drivers of ETP-ALL is correct?
A. NOTCH1 mutations are more common in ETP-ALL than in other T-cell ALL subtypes.
B. Recurrent 5q deletions result in deletion of the NR3C1 locus.
C. ETP-ALL blasts have lower mutational loads compared with blasts of other T-cell ALL subtypes.
D. Recurrent activating aberrations involve kinase-encoding genes.
Question 4
Which of the following statements about the prognosis of ETP-ALL is/are correct?
A. Patients with ETP-ALL have a higher frequency of measurable residual disease after therapy.
B. The use of contemporary risk-adapted regimens in children has improved outcomes.
C. There are fewer data available with regard to mitigating the adverse prognosis of ETP-ALL in adults.
D. All of the above.
Answers to Hematology Expert Review Questions
Question 1
Which of the following statements about immunophenotype in ETP-ALL is correct?
Correct answer: C. These leukemias do not express CD1a or CD8.
Expert Perspective
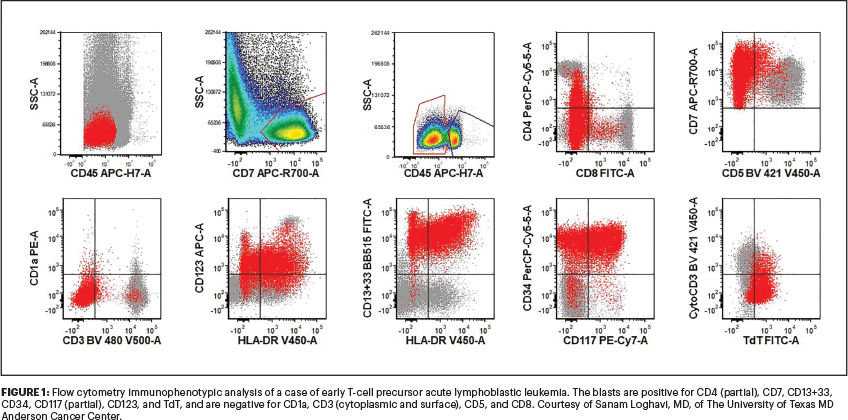
Early T-cell precursor acute lymphoblastic leukemia (ETP-ALL) is a neoplasm composed of cells committed to T-cell lineage but with a unique immunophenotype indicating only limited early T-cell differentiation.1-7 These leukemias are positive for CD7 and cytoplasmic CD3, are negative or dimly positive for CD5 (< 75% lymphoblasts), and express one or more stem cell or myeloid-associated markers, including CD11b, CD13, CD33, CD34, CD65, CD117 (KIT), or HLA-DR, in more than 25% of lymphoblasts. ETP-ALL is negative for CD1a, CD8, and myeloperoxidase. In aggregate, these immunophenotypic features are known as an early thymic phenotype (Figure 1).
Question 2
Which statement about the ETP-ALL cell of origin is correct?
Correct answer: D. The leukemia stem cells are committed to the T-cell lineage, and the leukemia is derived from T-cell precursors in the thymus.
Expert Perspective
ETP-ALL is thought to be derived from T-cell precursors in the thymus (not bone marrow) that have recently immigrated from the bone marrow and which still retain potential for myeloid and stem cell characteristics.
Question 3
Which statement about oncologic drivers of ETP-ALL is correct?
Correct answer: D. Recurrent activating aberrations involve kinase-encoding genes.
Expert Perspective
Genetic studies of ETP-ALL have shown that these leukemias have an unstable genome and are heterogeneous at the DNA level. ETP-ALL blasts have higher mutational loads compared with blasts of other T-cell ALL subtypes. NOTCH1 mutations and deletions of chromosome 9/CDKN2A mutations are less common in ETP-ALL compared with other T-cell ALL subtypes. Analysis of the prognostic significance of NOTCH activation in T-cell ALL has shown that NOTCH1 mutations may confer a better prognosis. Some ETP-ALL cases carry genomic aberrations that activate genes of the HOXA locus. Such activating events have been correlated with chemoresistance and inferior outcomes in adults with ETP-ALL.
Up to 75% of cases of ETP-ALL have cytogenetic abnormalities, including a high frequency of deletions involving chromosomal loci 5q, 11q, and 13q. Recurrent 5q deletions result in deletion of the NR3C1 locus encoding for the glucocorticoid receptor. Interestingly, recent evidence has shown that reduced glucocorticoid receptor expression can induce steroid resistance in T-cell ALL. Recurrent activating aberrations involving kinase-encoding genes, such as FLT3, NRAS, IL7R, JAK1, and JAK3, occur in ETP-ALL. Whole-exome sequencing in adult ETP-ALL also has shown a high rate of DNMT3A mutations.
Question 4
Which of the following statements about the prognosis of ETP-ALL is/are correct?
Correct Answer: D. All of the above.
Expert Perspective
Patients with ETP-ALL commonly present with high-risk clinical features and a higher frequency of measurable residual disease (MRD) after therapy. Although the kinetics of the response to therapy appear to be different in ETP-ALL compared with other T-cell ALL subtypes, the ultimate outcome in children using an MRD risk–adapted strategy may mitigate its negative prognostic impact. There are fewer data showing a similar favorable effect in adults.
DISCLOSURE: Dr. Abutalib has served on the advisory board for AstraZeneca. Dr. Medeiros reported no conflicts of interest.
REFERENCES
1. Borowitz MJ, Chan JKC, Bene MC, et al: Early T-cell precursor lymphoblastic leukaemia, in Swerdlow SH, Campo E, Harris NL, et al (eds): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, p 212. Lyon, France, International Agency for Research in Cancer, 2017.
2. Alaggo R, Amador C, Anognostopoulos I, et al: The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 36:1720-1748, 2022.
3. Coustan-Smith E, Mullighan CG, Onciu M, et al: Early T-cell precursor leukaemia: A subtype of very high-risk acute lymphoblastic leukaemia. Lancet Oncol 10:147-156, 2009.
4. Medeiros LJ: Early T-cell precursor lymphoblastic leukemia, in Ioachim’s Lymph Node Pathology, 5th ed. Philadelphia, Lippincott Williams & Wilkins, 2021.
5. Cordo’ V, van der Zwet JCG, Canté-Barrett K, et al: T-cell acute lymphoblastic leukemia: A roadmap to targeted therapies. Blood Cancer Discov 2:19-31, 2020.
6. Dunsmore KP, Winter SS, Devidas M, et al: Children’s Oncology Group AALL0434: A phase III randomized clinical trial testing nelarabine in newly diagnosed T-cell acute lymphoblastic leukemia. J Clin Oncol 38:3282-3293, 2020.
7. Jain N, Lamb AV, O’Brien S, et al: Early T-cell precursor acute lymphoblastic leukemia/lymphoma (ETP-ALL/LBL) in adolescents and adults: A high-risk subtype. Blood 127:1863-1869, 2016.
Dr. Abutalib is Director, Hematology and BMT/Cellular Therapy Programs; Director, Clinical Apheresis Programs Cancer Treatment Centers of America, Zion, Illinois; Associate Professor, Rosalind Franklin University of Medicine and Science; and Founder and Co-Editor of Advances in Cell & Gene Therapy. Dr. Medeiros is Professor and Chair, Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston.