
Women with atypical breast lesions have approximately a 5% to 11% risk of developing breast cancer within 5 years, depending on histology, and this risk can be reduced with chemoprevention, according to a presentation at the 2011 San Antonio Breast Cancer Symposium.1
 Investigators tracked the outcomes of 2,942 women with atypical breast lesions treated at Boston area hospitals. The study was led by Suzanne B. Coopey, MD, a surgical oncologist at Massachusetts General Hospital, Boston, and was presented by senior investigator Kevin S. Hughes, MD, also a surgical oncologist at Massachusetts General.
Investigators tracked the outcomes of 2,942 women with atypical breast lesions treated at Boston area hospitals. The study was led by Suzanne B. Coopey, MD, a surgical oncologist at Massachusetts General Hospital, Boston, and was presented by senior investigator Kevin S. Hughes, MD, also a surgical oncologist at Massachusetts General.
“While all types of atypical lesions are known to increase the risk of breast cancer, it is not clear from the medical literature just how much they increase risk, because there are conflicting data,” Dr. Hughes noted. “Also, the effect of chemoprevention in the clinical setting needs to be clarified.”
Large Population Analyzed
Dr. Coopey and colleagues reviewed 76,333 pathology reports for 42,950 individuals and identified 2,942 women (mean age 51) diagnosed with atypical breast lesions between 1987 and 2010. This included 1,199 (40.8%) with atypical ductal hyperplasia, 828 (28.1%) with atypical lobular hyperplasia, 570 (19.4%) with lobular carcinoma in situ, and 345 (11.7%) with borderline ductal carcinoma in situ/severe atypical ductal hyperplasia. The effect of chemoprevention was analyzed from 1999 forward.
After an overall follow-up of 67 months, breast cancer was diagnosed in 7.1% of women with atypical ductal hyperplasia, 10.9% with atypical lobular hyperplasia, 11.1% with lobular carcinoma in situ, and 8.4% with borderline ductal carcinoma in situ/severe atypical ductal hyperplasia. Median time to breast cancer diagnosis was 48 months, 50 months, 47 months, and 60 months, respectively. There were significantly more ipsilateral cancers for all atypical types combined (P < .005), and bilateral cancers were rare, Dr. Hughes reported.
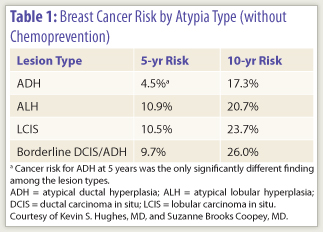
“The different diagnoses did not carry different levels of cancer risk,” he observed. “This is not what we expected when we started the study.” The breast cancer risks by type of atypia are shown in Table 1.
Invasive cancers were significantly more common than noninvasive cancers among patients with lobular carcinoma in situ (71.1%) and atypical lobular hyperplasia (68.9%) (P < .001) but were not more frequent for the other types of lesions (47.4% in atypical ductal hyperplasia and 57.1% in patients with borderline lesions), he said.
 Outcomes with Chemoprevention
Outcomes with Chemoprevention
Among the 2,460 patients diagnosed since 1999, chemoprevention with tamoxifen, raloxifene (Evista), and/or exemestane (for any duration) was received by 466 (18.9%), whereas 1,472 (59.8%) received no treatment. (Data were not available for 21.2% of patients.)
“Chemoprevention had a clear effect, significantly decreasing the risk of cancer occurrence for all atypia types,” Dr. Hughes reported. “But only 20% of patients took these medications, which certainly leaves room for improvement.”
At 5 years, cancer occurred in only 4.1% receiving some type of chemopreventive agent, vs 8.3% of patients left untreated. At 10 years, the difference widened, with cancer diagnosed in 7.5% vs 21.3% (P < .05).
By atypia type, for chemoprevention vs no treatment, the 10-year cancer risks were 8.5% vs 19.9% for atypical ductal hyperplasia, 8.5% vs 18.7% for atypical lobular hyperplasia, 2.1% vs 14.7% for borderline lesions, and 10.3% vs 32.4% for lobular carcinoma in situ. All were statistically significant (P < .05), he said.
Interest Sparked Discussion
Several questions from attendees followed the presentation, and discussion was lively. Dr. Hughes said his group hopes to mine the data to determine risk according to age, benefit of chemoprevention by duration of treatment, risk according to amount or magnitude of atypia, and other factors that might further delineate cancer risk and the value of chemoprevention.
Elaborating on the high incidence of noninvasive ductal carcinoma in situ (approximately 40%) diagnosed over time, Dr. Hughes noted that patients were closely followed with yearly mammograms. “The high rate of screening might explain this high rate,” he said.
When asked which patients should receive chemoprevention, he said, “I tend to use chemoprevention for any patient with atypia, though we need to decide if we can exclude patients age 70 and older.” He added that more needs to be learned regarding the safety of chemopreventive agents in patients with certain risk factors. ■
Disclosure: Drs. Hughes and Coopey reported no potential conflicts of interest.
Reference
1. Coopey SB, Mazzola E, Buckley JM, et al: Clarifying the risk of breast cancer in women with atypical breast lesions. 2011 San Antonio Breast Cancer Symposium. Abstract S4-4. Presented December 7, 2011.