

A variety of treatment options used today can achieve good outcomes in patients with mediastinal lymphomas, according to James O. Armitage, MD, the Joe Shapiro Professor of Medicine at the University of Nebraska Medical Center in Omaha. He discussed some of the current evidence helping to refine the management of primary mediastinal large B-cell lymphoma and mediastinal gray zone lymphoma at the Pan Pacific Lymphoma Conference held in Kohala Coast, Hawaii.
Primary Mediastinal Large B-Cell Lymphoma
“Mediastinal B-cell lymphoma is a unique entity…. It really is different from the rest of the diffuse large B-cell lymphomas,” Dr. Armitage pointed out.1 This tumor initially caught attention in part because of its distinct survival pattern, with nearly all relapses after remission occurring within 3 years. “In this disease, patients either get over it—and you know that in a relatively short period of time—or they succumb, and unfortunately, salvage therapy has not always been as effective as we would like. So it’s different from other large B-cell lymphomas,” he elaborated.
When it comes to treatment, a retrospective analysis of data from patients treated in Vancouver, British Columbia, found that CHOP-R (cyclophosphamide, doxorubicin, vincristine, and prednisone, with rituximab [Rituxan]) was superior to CHOP alone with respect to 5-year overall survival (88% vs 70%).2 Outcomes did not differ significantly between patients who did vs did not routinely get radiotherapy (82% vs 89%). Among patients undergoing positron-emission tomography (PET) at the end of CHOP-R, survival was statistically indistinguishable for the PET-positive group given radiotherapy and the PET-negative group not given radiotherapy (95% vs 89%).
“It looks like this certainly would provide an argument that if you want to use CHOP-R, you do a PET scan at the end, and if patients are PET-negative, you can follow them, and you end up with roughly a 90% survival, rather than giving radiotherapy to all of these patients. This would be one way to try to avoid giving radiotherapy,” Dr. Armitage noted.
The German MINT (MabThera International Trial Group) study compared CHOP-like chemotherapy with vs without rituximab in patients with diffuse large B-cell lymphoma, with radiotherapy added for most patients.3 In an analysis looking at tumor subtypes, the 87 patients with mediastinal large B-cell lymphoma had a poorer complete response rate if they did not receive rituximab, and rituximab also yielded a better 5-year overall survival (78% vs 90%).4
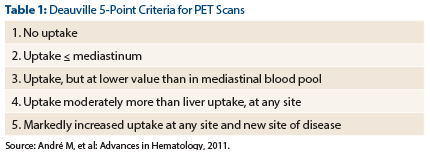
A retrospective analysis by the International Extranodal Lymphoma Study Group assessed the prognostic value of various PET cutoffs among patients with mediastinal large B-cell lymphoma who had been treated with rituximab and anthracycline-containing chemoimmunotherapy, and usually also radiotherapy.5 The best discrimination was seen for a Deauville score of 1, 2, or 3 vs a Deauville score of 4 or 5 (Table 1); this cutoff yielded a 99% negative predictive value for progression or relapse.
“Remember, PET scans are much more valuable in terms of negative predictive value than positive predictive value. When a PET scan is positive, there are more things than just lymphoma that can be causing it…. But a negative PET scan is more prognostic,” Dr. Armitage noted.
Finally, a study of patients with mediastinal B-cell lymphoma treated with dose-adjusted EPOCH-R (etoposide, doxorubicin, and cyclophosphamide with vincristine, prednisone, and rituximab) but no radiotherapy showed that this regimen achieved excellent outcomes. 6 With a median follow-up of 5 years, patients had an event-free survival of 93% and an overall survival of 97%. However, if it is administered in the hospital, this approach is more inconvenient and more expensive.
Current data thus show that a variety of approaches can achieve longer-term survival of approximately 90% in patients with this disease. “So is there only one way to treat mediastinal large B-cell lymphoma? I think the answer is no. However, if the goal is to avoid radiotherapy, this seems to be most likely achieved by using EPOCH-R” he said.
Mediastinal Gray Zone Lymphoma
“Mediastinal gray zone lymphoma is a real but confusing entity,” Dr. Armitage commented. “We cannot even agree on how to spell it (gray vs grey). This isn’t composite diffuse large B-cell lymphoma and nodular sclerosing Hodgkin lymphoma. Instead, mediastinal gray zone lymphoma appears to have some characteristics of one type and some of the other,” he continued.
“This complicates our management. I can’t imagine that I’m the only one who has been frustrated wondering whether these patients are better off treated like they have a large B-cell lymphoma or like they have a Hodgkin lymphoma,” he added. Some likely good news from the molecular perspective is that these tumors are almost always positive for both CD20, suggesting a role for rituximab, and CD30, suggesting a possible role for brentuximab (Adcetris).
At present, data are insufficient to know how best to treat mediastinal gray zone lymphoma, according to Dr. Armitage. In a study of patients given dose-adjusted EPOCH-R without radiation therapy having a median follow-up of 4 years, those with gray zone lymphomas had poorer outcomes than those with primary mediastinal B-cell lymphoma, in terms of progression-free survival (45% vs 90%) and overall survival (75% vs 100%).7 However, with the addition of radiotherapy after chemotherapy, the rate of progression-free survival improved to about 80% in the patients with gray zone lymphomas.
“So I believe that when you treat mediastinal gray zone lymphoma, most of these patients should get radiotherapy. That’s what I would recommend to my patients,” he said, while acknowledging that the topic remains controversial. ■
Disclosure: Dr. Armitage is a consultant for Genentech, GlaxoSmithKline, Roche, Seattle Genetics, Spectrum, and Ziopharm, and a Member of the Board of Directors for Tesaro.
References
1. Cazals-Hatem D, Lepage E, Brice P, et al: Primary mediastinal large B-cell lymphoma. A clinicopathologic study of 141 cases compared with 916 nonmediastinal large B-cell lymphomas, a GELA (“Groupe d’Etude des Lymphomes de l’Adulte”) study. Am J Surg Pathol 20:877-888, 1996.
2. Savage KJ, Yenson PR, Shenkier T, et al: The outcome of primary mediastinal large B-cell lymphoma (PMBCL) in the R-CHOP treatment era. 2012 American Society of Hematology Annual Meeting. Abstract 303. Presented December 10, 2012.
3. Pfreundschuh M, Trümper L, Osterborg A, et al: CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: A randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol 7:379-391, 2006.
4. Witzens-Harig M, Ho AD, Kuhnt E, et al: Primary mediastinal B cell lymphoma treated with CHOP-like chemotherapy with or without rituximab: 5-year results of the Mabthera International Trial Group (≤MInT) study. 2012 American Society of Hematology Annual Meeting. Abstract 1612. Presented December 8, 2012.
5. Martelli M, Ceriani L, Zucca E, et al: [18F]fluorodeoxyglucose positron emission tomography predicts survival after chemoimmunotherapy for primary mediastinal large B-cell lymphoma: Results of the International Extranodal Lymphoma Study Group IELSG-26 Study. J Clin Oncol 32:1769-1775, 2014.
6. Dunleavy K, Pittaluga S, Maeda LS, et al: Dose-adjusted EPOCH-rituximab therapy in primary mediastinal B-cell lymphoma. N Engl J Med 368:1408-1416, 2013.
7. Dunleavy K, Pittaluga S, Tay K, et al: Comparative clinical and biological features of primary mediastinal B-cell lymphoma (PMBL) and mediastinal grey zone lymphoma (MGZL). 2009 American Society of Hematology Annual Meeting. Abstract 106. Presented December 6, 2009.