
Through the Lens of Oncology History
A Century of Progress
The text and photographs on these pages represent the establishment of oncology as a viable medical specialty during the mid-1800s. The images and captions are excerpted from a four-volume series of books titled Oncology Tumors & Treatment: A Photographic History, by Stanley B. Burns, MD, FACS. To view additional photos from this series of books, visit burnsarchive.com.
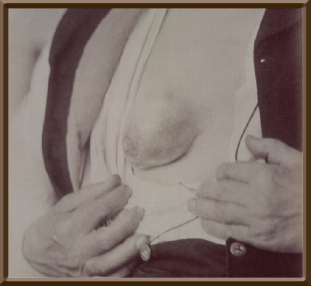
Tumors in the male breast, which are relatively rare, have always intrigued physicians. In Revue Médico-Photographique des Hôpitaux de Paris, Volume 6, 1874, an interesting photograph and case history of a breast neoplasm were presented in the section “Surgical Clinics.”
Mr. X… entered the Hospital ‘de Santé’ in the service of (Dr.) Demarquay with a diagnosis of tumor of the right breast. Three years prior, the patient had noted a small lump the size of a hazelnut. It was hard and did not change for a year. Suddenly, 2 years ago, the tumor started to develop. In 6 months, it was the size of an egg. It was now soft and mobile. The skin over the area was reddened but without inflammation. A second tumor began to develop next to the first. Both lesions began to grow, and the patient decided to consult Demarquay with the intention of having him remove the tumor. Examination indicated that a third tumor had appeared and the lesions appeared cystic. The ganglions (lymph nodes) in the armpit were not enlarged.
On May 19, 1873, at operation, Demarquay examined the protrusion. It was mobile and appeared to have three lobes. It measured 30 cm in circumference and was elevated 6 cm. The skin was red and firmly adherent to the tumor. A circular incision was made around the lesion and the tumor isolated. The content of the biggest cyst was emptied. Respecting and preserving the pectoralis muscle fibers, he dissected the tumor. Using seven small ligatures he tied off blood vessels. Six sutures closed the skin. A drain was placed in the wound. Postoperatively the patient did well until June 9.
June 7: Everything had gone well, and the drain was removed.
June 8: The sutures were removed.
June 9: A high fever was noted. The sides of the wound were now reddened.
June 10: Erysipelas became apparent, and the patient was treated with quinine sulfate. Dressings of glycerine applied to the wound.
June 11: Patient about the same. Glycerine dressings replaced by starch applications.
June 14: Erysipelas has now reached the arm. Despite the complications, the incision itself appears to be healing.
June 19: The wound is almost healed.
June 22: The patient’s fever drops a bit. The erysipelas has almost left the wound.
June 25: The wound has completely healed. There was no fever. Erysipelas has disappeared from the wound area and only remains in the lumbar region. The patient is now out of danger. Microscopic examination of the tumor indicated that the tumor was not malignant and appeared to be an adenoma. Preoperatively this was suggested by the absence of swollen armpit ganglions.
This case illustrates not only a breast tumor occurrence in a male, but the frequent infections that seemed a natural part of surgery. At this time, antiseptic operating principles were known but still not fully accepted.
In 1867, Sir Joseph Lister, MD, had described antiseptic techniques, but antisepsis was not generally used in Europe until the late 1870s. German surgeons were the first to adapt the procedure, which ultimately held, and led to their primacy in surgery at the end of the 19th century. ■
Excerpted from Oncology Tumors & Treatment: A Photographic History, The Anesthesia Era 1845-1875, by Stanley B. Burns, MD, FACS. Photograph courtesy of Stanley B. Burns, MD, and The Burns Archive.