
The ASCO Post is pleased to present Hematology Expert Review, an ongoing feature that quizzes readers on issues in hematology. In this installment, Drs. Syed Ali Abutalib and L. Jeffrey Medeiros explore the World Health Organization (WHO) classification of hematopoietic and lymphoid tissue malignancies, focusing on hairy cell leukemia. For each quiz question that follows, select the one best answer. The correct answers and accompanying discussions appear below.
Guest Editors

Syed Ali Abutalib, MD

L. Jeffrey Medeiros, MD
Dr. Abutalib is Associate Medical Director, Hematologic Malignancies and Stem Cell Transplant Program, City of Hope Chicago; and Founder and Co–Editor-in-Chief, Advances in Cell & Gene Therapy.
Dr. Medeiros is Professor and Chair, Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston.
Question 1
Which of the following statements about the epidemiology of hairy cell leukemia (HCL) is correct?
A. HCL is more commonly observed in Black than in White females.
B. The median age at diagnosis is 40 years.
C. HCL is not uncommon in children.
D. There is some evidence to support inherited susceptibility with HCL.
Question 2
Which of the following statements about clinical features and treatment of HCL is correct?
A. Generalized lymphadenopathy with massive splenomegaly are common findings at presentation.
B. Monocytopenia is a characteristic finding in HCL.
C. Bulky peripheral lymphadenopathy with pancytopenia are common findings at presentation.
D. Patients with HCL should be immediately treated at diagnosis.
Question 3
Which of the following phrases best describes the bone marrow morphology of HCL?
A. Focal nonparatrabecular nodular, interstitial or diffuse infiltrates of monotonous small round lymphocytes with scant cytoplasm
B. Focal nonparatrabecular and trabecular nodular or interstitial infiltrates of small- to intermediate-sized lymphocytes with variably condensed chromatin and irregular nuclear contours
C. Focal or extensive paratrabecular infiltrates with variable small cleaved lymphoid cells
D. Interstitial or diffuse infiltrate of small-sized lymphocytes exhibiting oval or indented nuclei with inconspicuous nucleoli, abundant pale cytoplasm, and reticulin fibrosis
Question 4
Which of the following features is most consistent with a diagnosis of HCL?
A. Splenomegaly and SOX11 expression by neoplastic B lymphocytes
B. Splenomegaly and CD5 and CD23 expression by neoplastic B lymphocytes
C. Splenomegaly and CD25 expression by neoplastic villous B lymphocytes
D. Splenomegaly and CD25-negative neoplastic villous B lymphocytes
Question 5
What percentage of patients with HCL present with hypocellular bone marrow?
A. < 2%
B. 10%
C. 30%
D. 40%
Answers to Hematology Expert Review Questions
Question 1
Which of the following statements about the epidemiology of hairy cell leukemia (HCL) is correct?
Correct answer: D. There is some evidence to support inherited susceptibility with HCL.
Expert Perspective
Hairy cell leukemia is a cytologically and immunophenotypically distinct, indolent neoplasm of small mature lymphoid cells with oval nuclei and abundant cytoplasm with so-called hairy cytoplasmic projections involving peripheral blood, splenic red pulp, and, in most cases, diffusely infiltrating bone marrow.1,2 The male-to female ratio is 4:1, and the incidence is substantially higher in White vs Black populations. Patients are predominantly middle-aged to elderly adults, with a median age of 58 years at diagnosis; HCL has been diagnosed rarely in patients in their 20s, but it is exceptionally uncommon in children.1 First-degree family members of patients with HCL have a higher-than-expected frequency of developing HCL, although the relative risk of such occurrence is lower compared with chronic lymphocytic leukemia (CLL).1,2
Question 2
Which of the following statements about clinical features and treatment of HCL is correct?
Correct answer: B. Monocytopenia is a characteristic finding in HCL.
Expert Perspective
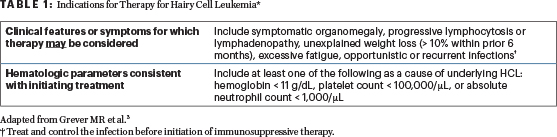
HCL represents ~2% of all leukemias. Approximately 10% to 25% of patients are asymptomatic at the time of diagnosis. However, the most common symptoms of HCL include weakness and fatigue, left upper quadrant pain, fever, and bleeding.1 Monocytopenia is a characteristic finding of HCL, with low-level involvement of the peripheral blood. Although most patients in the past presented with splenomegaly and pancytopenia, these findings appear to be much less frequent because of earlier detection of disease.2,3 In older literature, abdominal lymphadenopathy was often prominent, but lymphadenopathy is currently uncommon. Peripheral lymphadenopathy is uncommon at diagnosis (< 10%) and is usually not prominent. Downregulation of chemokine receptors such as CCR7 and CXCR5 explains the relative absence of lymph node involvement in HCL.1,2 Rarely, peripheral lymphadenopathy can be marked; the clinical significance of this occurrence is uncertain but may be related to transformation to a higher-grade process. Tumor cells are found predominantly in the bone marrow and spleen. Asymptomatic patients should be closely observed without therapy. The indications for therapy in HCL are shown in Table 1.
Question 3
Which of the following statements best describes the bone marrow morphology of HCL?
Correct answer: D. Interstitial or diffuse infiltrate of small-sized lymphocytes exhibiting oval or indented nuclei with inconspicuous nucleoli, abundant pale cytoplasm, and reticulin fibrosis.
Expert Perspective
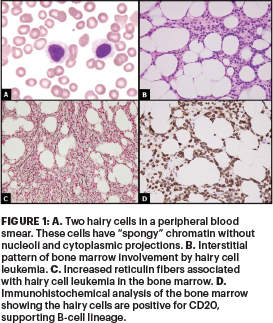
The diagnosis of HCL is best made on bone marrow biopsy. The extent of bone marrow effacement in HCL varies. The bone marrow core biopsy specimen (Figure 1) usually shows an interstitial or diffuse infiltrate of lymphoid cells. The primary pattern is interstitial or patchy, with some preservation of fat and hematopoietic elements. The infiltrate is characterized by widely spaced lymphoid cells with oval or indented nuclei. The wide spacing is attributable to the cells having abundant cytoplasm, in contrast with the closely packed nuclei of most other indolent lymphoid neoplasms involving the bone marrow. The abundant cytoplasm and prominent cell borders may impart a so-called fried-egg or honeycomb appearance. Mitotic figures are virtually absent.
When infiltration is minimal (such as in an early stage of disease), the subtle clusters of hairy cells can be easily overlooked. An increase in reticulin (not collagen) fibers is associated with all hairy cell infiltrates in bone marrow and other sites and often results in a so-called dry tap of the bone marrow. However, even if the needle contains only one or two small drops of material, often this material is rich in hairy cells. The hairy cells usually resemble those seen in the peripheral blood smears, except that the surface villous projections may be absent, and many cell nuclei are stripped of their cytoplasm. Choices A, B, and C best describe the bone marrow morphology of CLL, mantle cell lymphoma, and follicular lymphoma, respectively.
Question 4
Which of the following features is most consistent with a diagnosis of HCL?
Correct answer: C. Splenomegaly and CD25 expression by neoplastic villous B lymphocytes.
Expert Perspective
According to the WHO 5th edition classification,1 choice C favors the diagnosis of HCL. The classic immunophenotypic profile of HCL consists of bright monotypic surface immunoglobulin; bright co-expression of CD20, CD22, CD11c, and VE1 (a BRAF V600E stain); and expression of CD103, CD25, CD123, TBX21 (also called TBET), annexin A1, FMC7, CD200, and cyclin D1 (weak and nonuniform in ~50% of cases). Cyclin D1 is downstream of the MAPK-ERK pathway, and overexpression in HCL is a physiologic response, but hairy cells do not carry t(11;14)(q13;q32). Annexin A1 is the most specific marker for HCL but must always be compared with staining for a B-cell antigen (eg, CD20), because annexin A1 is also expressed by myeloid cells and a proportion of T cells.
DBA.44 is another antibody that reacts with almost all cases of HCL but is not specific for HCL. CD5 and CD10 are usually negative, but rare (< 5%) cases that express either antigen have been described. Somatic BRAF V600E mutation is present in virtually 100% of patients with HCL. Immunohistochemical staining for V600E-mutant BRAF protein can be helpful and may be useful for recognizing residual disease after therapy. CD25 and tartrate-resistant acid phosphatase expression is induced by BRAF V600E mutation. Choices A, B, and D favor the diagnosis of mantle cell lymphoma, CLL, and splenic B-cell lymphoma or leukemia with prominent nucleoli, respectively.
Question 5
What percentage of patients with HCL present with hypocellular bone marrow?
Correct answer: B. 10%.
Expert Perspective
Approximately 10% of patients will have a hypocellular bone marrow biopsy at diagnosis, reflecting a decrease in normal hematopoiesis. This finding can lead to an incorrect diagnosis of aplastic anemia. In such cases, immunostaining for a B-cell antigen such as CD20 is essential for the identification of an abnormal B-cell infiltrate, prompting the use of immunohistochemical stains more specific for HCL.
DISCLOSURE: Dr. Abutalib has served on the advisory board for AstraZeneca. Dr. Medeiros reported no conflicts of interest.
REFERENCES
1. Alaggio R, Amador C, Anagnostopoulos I, et al: The 5th edition of the World Health Organization classification of haematolymphoid tumours: Lymphoid neoplasms. Leukemia 36:1720-1748, 2022.
2. Medeiros LJ: Ioachim’s Lymph Node Pathology, 5th edition, pp 442-451. Philadelphia, PA; Wolters Kluwer; 2021.
3. Grever MR, Abdel-Wahab O, Andritsos LA, et al: Consensus guidelines for the diagnosis and management of patients with classic hairy cell leukemia. Blood 129:553-560, 2017.