
The ASCO Post is pleased to continue this occasional special focus on the worldwide cancer burden. In this issue, we feature a close look at the cancer incidence and mortality rates in Botswana. The aim of this special feature is to highlight the global cancer burden for various countries of the world. For the convenience of the reader, each installment will focus on one country from one of the six regions of the world as defined by the World Health Organization (ie, Africa, the Americas, Southeast Asia, Europe, Eastern Mediterranean, and Western Pacific). Each section will focus on the general aspects of the country followed by the current and predicted rates of incidence and cancer-related mortality. It is hoped that through these issues, we can increase awareness and shift public policy and funds toward proactively addressing this lethal disease on the global stage.

Botswana is a southern African country bordering Zimbabwe, Namibia, and South Africa. Botswana gained its independence in 1966 and has since maintained a democratic government. It has one of the most stable economies in Africa, heavily supported by the coal and diamond mining industry. It has a population of 2.3 million people, with a population growth rate of 1.5%, and the median age is 25.7 years. The current health expenditure is 6.1% of the gross domestic product. The country has a physician density of 0.53 and a hospital bed density of 1.8 beds per 1,000 population. Princess Marina Hospital is the largest government-funded hospital in the country and is located in the capital city, Gaborone.
Health Concerns
The HIV/AIDS epidemic in the 1990s greatly affected the country’s public health, threatening the life expectancy to 40 years by the 2000s. The Centers for Disease Control and Prevention initially partnered with the government of Botswana in 1995 with the focus of tuberculosis prevention; however, the partnership expanded shortly thereafter to focus on HIV testing and treatment. The incidence and mortality of HIV/AIDS have consistently decreased since the mid-1990s, and the coverage of people receiving antiretroviral therapy continues to increase, achieving more than 97% viral load suppression among those receiving antiretroviral therapy.
GUEST EDITORS

Chandrakanth Are, MBBS, MBA, FRCS, FACS

Emily Zurbuchen, MD
Despite the country’s successful treatment of HIV, HIV/AIDS remains the number-one cause of death, followed by ischemic heart disease and stroke. Cancer does not make the top 10 causes of death in this country; however, it is a climbing health concern for the county.
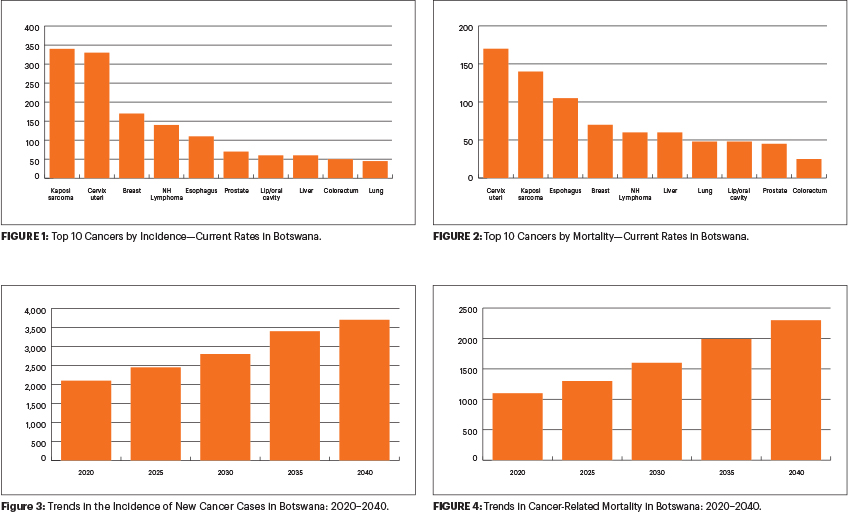
The Botswana National Cancer Registry was developed in 1999, and the first cancer report was produced in 2005, which captured 2,000 malignant cases between 1986 and 2004. The incidence of cancer is expected to rise from 1,953 in 2018 to 3,760 in 2040, whereas mortality is expected to increase form 1,064 in 2018 to 2,284 in 2040.
Current Cancer Trends and International Partnerships
The county’s experience with the HIV epidemic and its successful management has influenced its current cancer trends. With successful treatment of HIV, the country is seeing an aging population burdened by chronic infection and associated cancers. Kaposi sarcoma, cervical cancer, and breast cancer are the most common cancers by incidence, whereas cervical cancer, Kaposi sarcoma, and esophageal cancer are the most common causes of cancer-related mortality. The top-two cancers by incidence and mortality are Kaposi sarcoma and esophageal cancer in men and cervical and breast cancers in women.
The Botswana–Harvard AIDS Institute Partnership (BHP) was formed amid the HIV epidemic to assist in dealing with the high incidence of HIV. With the success of HIV management and the development of HIV-opportunistic cancers, the need for assistance in the management of these cancers arose.
Formed in 2001, the Botswana–UPenn Partnership (BUP) aims to promote and improve health care by using an interdisciplinary approach to promote research as well as to provide clinical care through funding relief. One of its clinical areas of focus was cervical cancer, including measures such as screening programs, increasing awareness, promoting treatment, and vaccination efforts.
A collaborative effort with the Massachusetts General Hospital led to the formation of the Botswana Oncology Global Outreach (BOTSOGO) in 2011. Through BOTSOGO, a brachytherapy facility was created; it treats about 60 patients with cervical cancer per month. A pediatric oncology program was developed in 2007 from the collaboration among the Botswana government, Baylor College of Medicine, and Texas Children’s Hospital.
In August 2018, Rutgers Global Health institute and the government of Botswana collaborated to launch the Botswana–Rutgers Partnership for Health, with the goal of transforming cancer care and prevention. The pinnacle of this partnership is telementoring, which allows physicians in Botswana access to medical opinions from experts. Areas of improvement identified during this partnership include delays in cancer diagnosis, lack of public health prevention strategies, deficiencies in medications, and shortages in the specialty-trained workforce.
Botswana has a unique history of cancer trends heavily influenced by the prevalence of HIV. The country has demonstrated its success in management of HIV, and it is hoped that ongoing partnerships will also replicate that success in cancer care.
DISCLOSURE: Dr. Are is a board member with Global Laparoscopy Solutions Inc; has received research funding from Pfizer; and has a patent with the University of Nebraska Medical Center for a laparoscopy instrument. Dr. Zurbuchen reported no conflicts of interest.
ADDITIONAL READINGS
1. https://www.cia.gov/library/publications/the-world-factbook/geos/bc.html
2. https://www.who.int/countries/bwa/en/
3. https://www.who.int/cancer/country-profiles/bwa_en.pdf
4. https://www.cdc.gov/globalhealth/countries/botswana/default.htm
5. https://afcrn.org/membership/members/118-bncr
7. https://globalhealth.rutgers.edu/where-we-work/botswana/
8. https://www.unaids.org/en/regionscountries/countries/botswana
9. https://www.cdc.gov/globalhivtb/where-we-work/Botswana.pdf
10. https://medicalxpress.com/news/2019-03-cancer-botswana.html
11. http://www.xrt.upenn.edu/DeptRadOncBotswanaInitiative.html#
12. Grover S, Raesima M, Bvochora-Nsingo M, et al: Cervical cancer in Botswana: Current state and future steps for screening and treatment programs. Front Oncol 5:239, 2015.
13. Slone JS, Slone AK, Wally O, et al: Establishing a pediatric hematology-oncology program in Botswana. J Glob Oncol 4:1-9, 2018.